Category: Role of psychologists
Posted by Dr. El - March 13, 2020 - McKnight's Long-Term Care News, Resident care, Role of psychologists


As the number of coronavirus cases increases around the world, providers may be worried about the emotional impact of the outbreak on residents and how to handle it. One would expect residents to be concerned, given that they’re at higher risk due to their ages, underlying health problems and residence in a communal setting.
Rather than mass panic, my experience and an informal query of my psychologist colleagues suggests that they may not be as worried as you’d think. As of last week, remarkably few of them have raised the issue in psychotherapy sessions (where uneasiness of every kind is discussed).
My colleagues and I speculate that the majority of residents are not unduly alarmed about the situation due to a combination of factors: more pressing problems, successful passage through many prior hardships, fatalism (i.e., “At this age, something’s going to get me”), denial (“it’s happening far away”), and trust that the facility will keep them safe.
Nevertheless, despite their general calm and resilience, it’s perfectly reasonable for residents to have questions and concerns. There will be some who are deeply unsettled by the prospect of the virus, particularly those with anxiety disorders and people struggling with depression. There may also be individuals who have had past traumatic experiences with hospital-acquired infections, isolation precautions, or communicable illnesses such as polio.
Facilities are no doubt reviewing infection control procedures and holding staff education sessions for their employees. To address the emotional needs of residents, add a brief segment to staff training that includes the following suggestions:
- Limit the amount of time residents spend watching the news. There’s no need for them to be exposed to hours of alarming reports on the day room television.
Posted by Dr. El - May 6, 2019 - Business Strategies, Common Nursing Home Problems and How Psychologists Can Solve Them, Communication, McKnight's Long-Term Care News, Role of psychologists

The top recommendation in the April 9 McKnight’s article “Researchers share 6 tips to improve nursing home care for blacks and Latinos” was to include a social worker on staff in the facility. “Great,” a reader commented, but “ask CMS … if they will pay for it.”
Perhaps, though better yet, social workers will pay for themselves.
A study published in March discussed the role and value of social work staff, with the surprising finding that deficiency scores are reduced twice as much when there’s an increase in social service staffing as compared to an increase in nursing staff. Lower deficiency scores can translate into better CMS star ratings and increased admissions, as well as reduced liability risk, creating a financial savings worth the price of a social worker salary.
The research brief goes on to report that while there’s been an increase in staffing in many other departments over time, the number of social workers remains low. The authors also note that there are no mandated qualifications for social work staff but that when social workers have higher qualifications such as a master’s degree, resident outcomes improve.
Interestingly, the other department that had almost as much effect on improving deficiency scores was the activities department, another psychosocially focused part of the team. (They didn’t study consulting psychologists, but I’d like to think we would have helped as well!)
For the entire article, visit:

Posted by Dr. El - April 18, 2019 - McKnight's Long-Term Care News, Nominations/Awards, Role of psychologists

Here’s my latest article on McKnight’s Long-Term Care News:

“My column won a bronze award for best blog in the 2019 American Society of Healthcare Publication Editors competition,” I informed a friend of mine, “but I feel funny telling people.”
“Women have such a hard time with this!” she said with some exasperation. “You HAVE to tell them, Eleanor. Who else is going to let them know but you?”
With her words in mind I posted about it on LinkedIn, Facebook, Twitter and my main psychology group, Psychologists in Long-Term Care. I received many wonderful, supportive, unexpected replies. I wasn’t going to write about it for this column (because, gosh, wasn’t that enough already?), but I decided to for several reasons.
I view part of my job as a psychologist as being a role model. On the units, I’m aware that the aides and my other co-workers are observing how I speak to them and to the residents and families. Similarly, in writing this column, I represent psychology to those who work in long-term care management. If people, particularly women, find it difficult to talk about their accomplishments, then perhaps I can model sharing an achievement in order to encourage more colleagues to do the same.
Dealing with extensive regulations, reimbursement challenges, elaborate documentation requirements and a punitive environment can erode the joy of helping elders. Acclamation for accomplishments, on the other hand, can bring joyfulness back to the job. I could have told just my mother and while that would have been nice, by sharing it with a larger group, the positive response is magnified, giving me added energy to continue my work. I’m sure there’s a scientific, dopamine thing happening, but the gist is that it feels good to be acknowledged. The reverse is true as well: Offering a genuine compliment can make the giver feel better too.
For the entire article, visit:

Posted by Dr. El - November 12, 2018 - Common Nursing Home Problems and How Psychologists Can Solve Them, Psychology Research Translated, Resident care, Role of psychologists
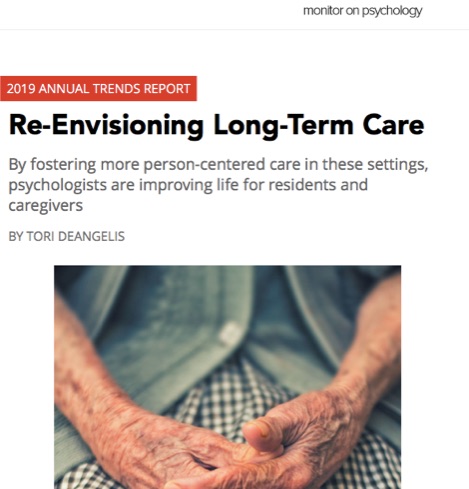
The American Psychological Association published an article in the APA Monitor on “Trends to Watch in 2019.” I was pleased to see that geropsychology was Trend #5. Read what my colleagues and I have to say in Tori DeAngelis’ piece on Re-Envisioning Long-Term Care.
Posted by Dr. El - October 7, 2018 - Anecdotes, Depression/Mental illness/Substance Abuse, McKnight's Long-Term Care News, Personal Reflections, Role of psychologists, Something Good About Nursing Homes

Here’s my latest article on McKnight’s Long-Term Care News:
“No,” Diane said when I showed up at her door for our Thursday session. “I don’t want to talk to you. I’m too aggravated.” She turned her head and looked out the window for a moment.
“I’m surprised.” I replied. “We had such a nice conversation the last time. Plus, being aggravated is a perfect reason to talk to the psychologist.”
She looked back at me and sighed with exasperation, “Fine! Sit down. But I’m not going to be very good company.”
“You don’t have to be a star, baby, to be in my show.” I sang the refrain to the old song, mostly on tune.
She rolled her eyes. “They’re driving me crazy here,” she began, launching into an account of her recent fall on the way to the bathroom. “And now they won’t let me do anything by myself! They’re always yelling at me to wait for them, but then they don’t come when I call for them.”
It was the same tale I’d heard from two residents in my other facility that week.
********
Maya was a frail woman in her late 70s who navigated around her room with a walker. She spent most of her time alone, crocheting colorful booties that she carefully tied onto the walker frame, which served as a display for her wares.
“Five dollars each,” she told me, when I commented on her handiwork. Her earnings, I learned several sessions later, were going to her disabled son, who came to the nursing home every few weeks to collect the money she’d made for him. “He’s a good boy,” she assured me.
Maya had been placed on the dementia unit, though she didn’t have dementia. Residents wandered in and out of her room, touching her yarn and the slippers. She yelled at them to stop, leading to chart notes saying she was agitated and eventually to a move to a different floor.
Once among residents more similar to herself and assigned to a consistent, experienced aide who took her under her wing, Maya’s mood and behavior improved considerably and we discussed concluding our sessions. I arrived for our last meeting with a $5 bill in hand and left with a beautifully crocheted pair of booties I didn’t need.
For the entire article, visit:

yarn in apile
Posted by Dr. El - July 29, 2018 - Books/media of note, Personal Reflections, Role of psychologists, Talks/Radio shows

NursingAssistantGuides.com, an educational site for certified nursing assistants, has a new podcast series featuring experts in the field of geriatrics and long-term care. The podcasts offer the chance for those considering or working toward becoming a nursing assistant to get insider information about the field. I was pleased to be interviewed by registered nurse Patricia Laramee about mental health and elder care for their most recent podcast.
To listen, click HERE and be sure to check out the other excellent podcasts on this page.

Patricia Laramee, RN of NursingAssistantGuides.com
Posted by Dr. El - April 27, 2018 - Business Strategies, Customer service, Depression/Mental illness/Substance Abuse, McKnight's Long-Term Care News, Resident care, Role of psychologists, Stress/Crisis management, Transitions in care

Here’s my latest article on McKnight’s Long-Term Care News:

In Editorial Director John O’Connor’s April 16th column, he reported on a study from the Kaiser Family Foundation indicating that increasing numbers of new residents have dementia, are more physically ill and are more likely to be on psychoactive medications.
The study showed that there has been a shift away from long-term services and toward short-term rehab treatment. O’Connor noted the pressure that this puts upon facilities to provide high-quality care in the midst of the churn of residents.
There are many difficulties that can arise from this shift in pace and population, but I’ll focus here on the mental health aspects and their effects on nursing facilities.
One problem that occurs when the length of stay decreases is that the team has a shorter period in which to get to know their residents. They are less likely to notice subtle changes in behavior and mood and they have less time to make the type of personal connection that reassures residents.
Adding to this, the fact that many facilities are operating short of staff in an environment of high employee turnover creates a “perfect storm” of emotional neglect.
Residents enter long-term care facilities in distress. When I adapted the classic Holmes-Rahe Stress Inventory to the circumstances of nursing home admission, I found that residents are experiencing a level of stress considered to be a “life crisis” that puts them at a high risk for further health breakdown. Their families also tend to be in crisis.
Residents and their family members are likely to expect that when they enter long-term care, staff members will provide compassionate medical treatment. Instead, what they frequently find are stressed out nurses and overworked aides who have just enough time to dispense medications or to make up a bed, but none to sit and talk with an understandably anxious resident and their family members about what they can expect regarding their stay and their future.
Social workers — most of whom got into the field in order to provide such counsel — are now buried under a flood of admissions and discharges. They cannot offer emotional sustenance when they need to complete the paperwork on three new admissions and order a walker for the lady whose family wants to take her home tomorrow because her insurance coverage ran out.
It is impossible for direct care staff to provide the same level of service that they did prior to this change in acuity and length of stay. In turn, distress over providing suboptimal care contributes to staff turnover, exacerbating the problem.
For the entire article, visit:

Posted by Dr. El - February 15, 2017 - Business Strategies, Common Nursing Home Problems and How Psychologists Can Solve Them, Communication, Customer service, McKnight's Long-Term Care News, Resident education/Support groups, Role of psychologists, Transitions in care

Here’s my latest article on McKnight’s Long-Term Care News:
Long-term care has an image problem. For a variety of reasons, we aren’t associated with good times. There are things we can do to turn this around, though, starting with the perceptions of our residents.
Most people who come to live in a long-term care facility struggle with a sense of failure. This isn’t because of anything that occurred in their lives prior to placement, but because many people view living in a nursing home as a sign of a failed life.
The most common comment I’ve heard from new long-term residents over the years is, “I never thought I’d end up in a place like this.” Some add, “Where did I go wrong?”
There are good reasons for providers to address the inherent sense of failure many residents feel in LTC placement: It can increase customer satisfaction, improve morale among residents and staff, and reduce depression among residents, thereby lessening the need for antidepressants.
The role of the psychologist
Part of my job as a psychologist is to help residents recognize that living in a long-term care facility isn’t a failure. It’s not a reflection of a life poorly lived or necessarily indicative of difficulties in their relationships with their children or other loved ones.
I do this in several ways, depending on the person and the circumstances.
I start by telling residents that I regard it largely as a societal problem. We’ve made advances in healthcare that allow people to live longer with chronic illnesses, but we haven’t yet devoted the resources needed to help people manage successfully at home and to support their caregivers. Long-term care is often the best solution under the circumstances.
Sometimes offering that view is enough to make them feel better about the situation, but other times more is needed. For example, Marie was a new resident who’d worked as an aide in a psychiatric hospital. She was distressed about living in the nursing home and had become irritable and withdrawn. I took her to visit a well-adjusted resident, Linda, who’d been a coworker and a union representative at the same psych hospital. They talked about the old days for 20 minutes and never visited together again, but Marie had a new acceptance for placement — if the nursing home was good enough for Linda the union rep, it was good enough for her too.
As a neutral party, I can provide the perspective that families and facilities can’t, pointing out, for example, how hard family members have worked to keep them out of the facility for as long as they did, how their relationships can reset once someone else is in charge of hands-on caregiving, and the benefits of living in a communal environment with easy access to medical staff and activities.
Organizational component
Aside from referring residents for psychology services, facilities can address this aspect of their image problem in several ways:
For the entire article, visit:

Posted by Dr. El - November 10, 2016 - Communication, Depression/Mental illness/Substance Abuse, McKnight's Long-Term Care News, Resident care, Role of psychologists, Stress/Crisis management
Here’s my latest article on McKnight’s Long-Term Care News:
In preparing for a webinar on suicide prevention, I came across startling statistics about suicide rates among older adults. Despite the concern we often hear about teen suicide, the rate for elders is even higher.
While older adults make up 12% of the U.S. population, they account for 18% of all suicide deaths. In 2014, the highest suicide rate in the U.S. population (19.3 per 100,000 people) was among people 85 years or older.
In addition, elder suicide may be under reported by 40% or more. Not counted are “silent suicides,” like deaths from overdoses, self-starvation or dehydration, and “accidents.”
Training staff to assess suicide
Given its prevalence, it’s important for long-term care staff members to know how to recognize and address suicidal thinking and behaviors.
As a psychologist who’s been assessing suicidality since my teen years as a peer counselor in college, I feel comfortable with the process. Most facility staff members, however, haven’t had extensive training and are understandably anxious about an issue that’s likely to be out of their area of expertise. This can lead to over-caution, such as unnecessary one-to-one observation, or to missing signs of distress.
Staff training programs should educate team members about factors increasing the likelihood of depression and thoughts of suicide. Many of these influences are prevalent in our elderly population, such as physical illness, pain, functional impairment, losses and social disconnectedness.
Make use of consulting psychologists by referring residents for evaluation after losses and a decline in condition such as a downgrade in diet from chopped to pureed food, a limb loss, a move from a wheelchair to a reclining chair or a death in the family.
Team communication and support
Virtually all workers know it’s necessary to inform the charge nurse and other personnel about direct statements such as “I want to kill myself,” but staff members should be trained to look for other warning signs of potential suicide, which include changes in grooming, loss of interest in previously appealing activities, giving away possessions and making statements like, “I won’t be needing any more appointments.”
For the entire article, visit:
Posted by Dr. El - October 4, 2016 - Anecdotes, Depression/Mental illness/Substance Abuse, Inspiration, Role of psychologists
 Mabel was in her late 80s, had lost a leg to diabetes and didn’t hear well. She’d been suicidal upon her admission to the nursing home, but the team had worked hard to stabilize her mood. Months later, she wasn’t exactly happy, but she and Liza, her young private aide, attended activities together and she no longer thought she’d be better off dead.
Mabel was in her late 80s, had lost a leg to diabetes and didn’t hear well. She’d been suicidal upon her admission to the nursing home, but the team had worked hard to stabilize her mood. Months later, she wasn’t exactly happy, but she and Liza, her young private aide, attended activities together and she no longer thought she’d be better off dead.
I focused on her strengths when I was with her, appealing to her best self and trying to coax her out of her negativity. I frequently updated her on the news, giving her a report tailored to her interests.
“What do you think of this, Mabel?” I asked, sharing the latest events on the presidential election.
“I think it’s disgusting,” she replied.
“So are you ready to vote when they come around with the absentee ballot?”
“I’m not going to vote.”
“What?! Why not?” I asked, genuinely shocked.
“I’m not going to be alive to see it. Why should I care?”
“What about me?! What about Liza? She’s been awfully nice to you. Surely you can vote for Liza.”
Mabel paused and considered. “Yes. I can vote for Liza.”
A few days later I saw Liza and Mabel out of her bedroom talking to some other residents. Mabel was animated and actually smiling, a rare occurrence since I’d known her.
I’m sure a number of things contributed to Mabel’s shift in mood, but I have no doubt that recognizing her continued value as a citizen and having the opportunity to help Liza were among them.